

The success of direct acting antivirals (DAAs) could provide a cure for the majority of patients with hepatitis C virus (HCV) infection and could pave the way to eliminating the virus completely, according to Raymond Chung, MD, chief of hepatology and director of the Liver Center at Massachusetts General Hospital and professor of medicine at Harvard Medical School.
DDW News spoke with Dr. Chung about the opportunities and challenges that remain for gastroenterologists and hepatologists treating HCV.
DDW: With the success of DAAs, what are the remaining unmet needs?
Chung: We have curative therapies that can achieve a sustained virologic response (SVR) —essentially a cure — in nearly 100% of patients. So, in this regard, we’ve solved the science. However, there are subsets of patients who continue to experience slightly lower response rates. These include:
- Certain HCV subtypes, such as HCV genotypes 4r, 1l and 1p, principally found outside the U.S.
- Patients with decompensated cirrhosis. There aren’t many safe options in the context of decompensation. The hope is that patients can receive a liver transplant or other treatment to improve their hepatic function and then receive DAAs.
- Patients with hepatocellular carcinoma (HCC). Studies suggest that cure rates are lower in patients with active HCC. It’s been suggested viral reservoirs within the tumor render the virus inaccessible to DAAs. We may therefore wish to treat the HCC before giving DAAs to maximize our likelihood of success against the virus.
DDW: What considerations remain in a patient who does achieve an SVR?
Chung: There is a notion that curing a patient of their HCV should mitigate the risk of HCC. However, in patients with advanced liver disease, we see that the risk of HCC is substantially reduced — but not eliminated — after SVR.
It’s very important to remind patients that we’re not done after cure. This message sometimes gets lost when patients transition from their hepatologist or gastroenterologist to their primary care provider (PCP). There is a relatively sizable portion of cirrhotic patients at risk for HCC. We must continue HCC screening in these patients and ensure they don’t compromise their success by engaging in activities that increase their risk of HCC. Unfortunately, we currently don’t have the tools to stratify patients to know when, if ever, we can stop screening in these patients.
DDW: Do you think we have the ability to eliminate HCV?
Chung: We can certainly achieve elimination. However, despite the availability of curative regimens, the prevalence of HCV remains stubbornly high — new infections continue to outnumber cures. We need to meet the infection where it is by comprehensively identifying and treating it. If we are to fully eliminate HCV, we will also need a protective vaccine. No infectious disease in humans has ever been eliminated without an effective vaccine.
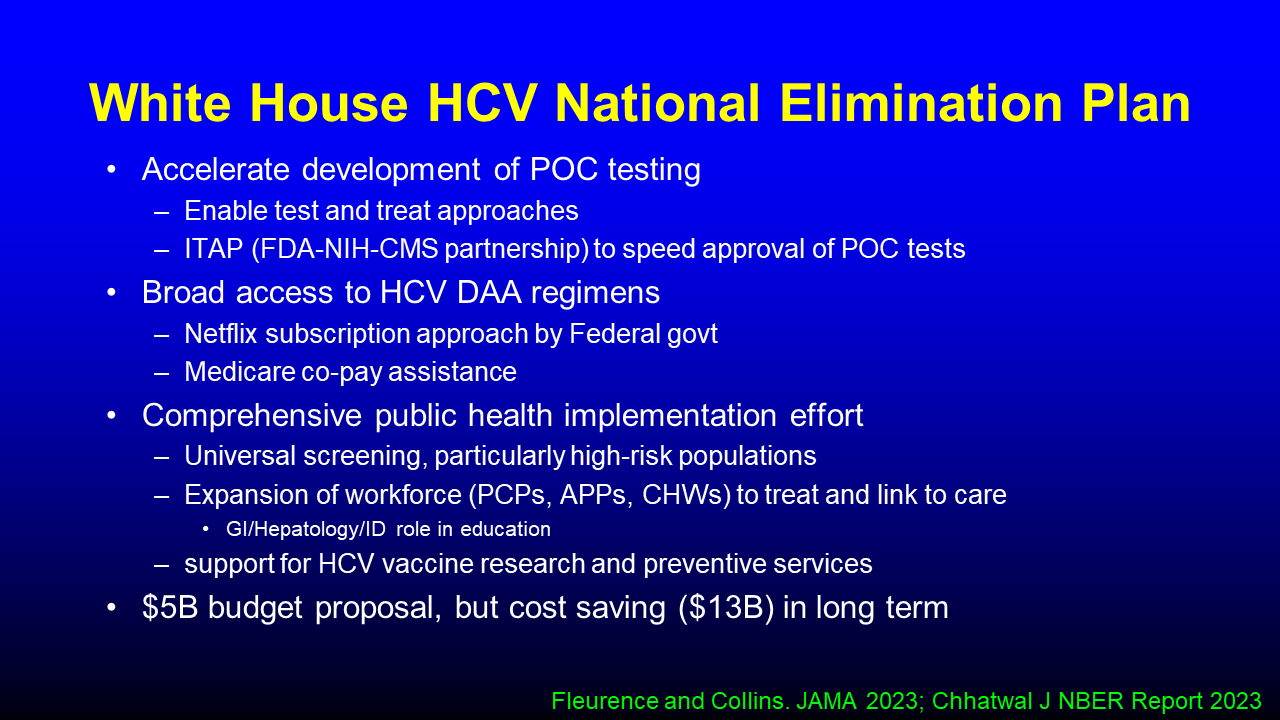
I am incredibly heartened to see the White House’s recent National Hepatitis C Elimination Program to eliminate HCV by 2030. The plan addresses all the key factors for full-blown implementation of the cure agenda, including:
- Enhancing diagnosis and accelerating the development of test-and-treat strategies.
- Enabling broad access to DAAs in at-risk populations.
- Funding comprehensive public health efforts to train and expand the work force involved in treating HCV.
- Supporting research for a protective HCV vaccine.
DDW: How can gastroenterologists and hepatologists contribute to elimination efforts?
Chung: Elimination is in our sights. It is now up to our community to educate others about liver disease and make sure we don’t declare victory too early with DAA cure. Counsel your patients and colleagues in primary care on the need for continued surveillance for HCC and to minimize harm to the liver by mitigating other HCC risk factors. We can and should also be involved in helping to expand the workforce by assisting in educational and training efforts.
Dr. Chung’s oral presentation, “Hepatitis C in 2023 – What you need to know” on Monday, May 8, at 8:50 a.m. CDT is part of the session “AASLD Hepatology for Gastroenterologists Symposium.”
If you’re attending DDW, your registration includes access to a recording of this session, available to watch at your convenience until May 17, 2024. Session captures will be released 24 hours after the session ends. Non-attendees can also purchase access to DDW On Demand to watch session recordings after DDW ends.